


Thoughts on the Clitoral Nerve "Hook-up" in Phalloplasty
Let's get back to basics and reason from first principles

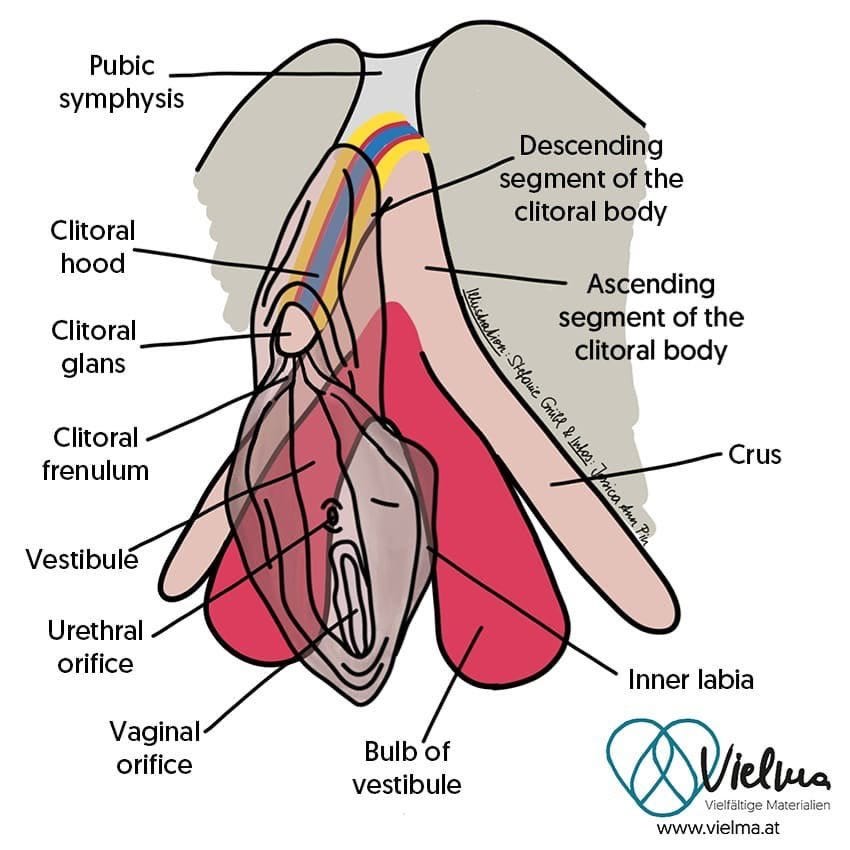
I'll let this doctor explain what they're cutting. To do phalloplasty nerve hookup, according to this purported expert, witch comports with other sources I've discussed in past videos, phalloplasty surgeons are severing one of the two dorsal clitoral nerves from the organ it innervates. They're taking a scalpel and cutting the nerve that supplies a significant portion of the clitoris, away from the clitoris.
If you sever one of the two recurrent laryngeal nerves, you will lose function in part of your voice. Your voice will become weakened or fully paralyzed on that side. The other side won't grow to compensate for it. Laryngeal nerve grafts require surgery. Eagle syndrome affects my vagus nerve including superior and recurrent branch, causing neuropathy that means my voice is sometimes hoarse from walking too much in one day.

The vagus nerve wanders. Richard Dawkins famously demonstrated this by dissecting a giraffe, which is the infamous new atheism to speech-language pathology pipeline that I fell victim to as an impressionable teenager.
Depending on where there is a lesion on the recurrent laryngeal branch of the vagus nerve, and which one you choose (right vs. left) you may also end up with elevated heartrate.
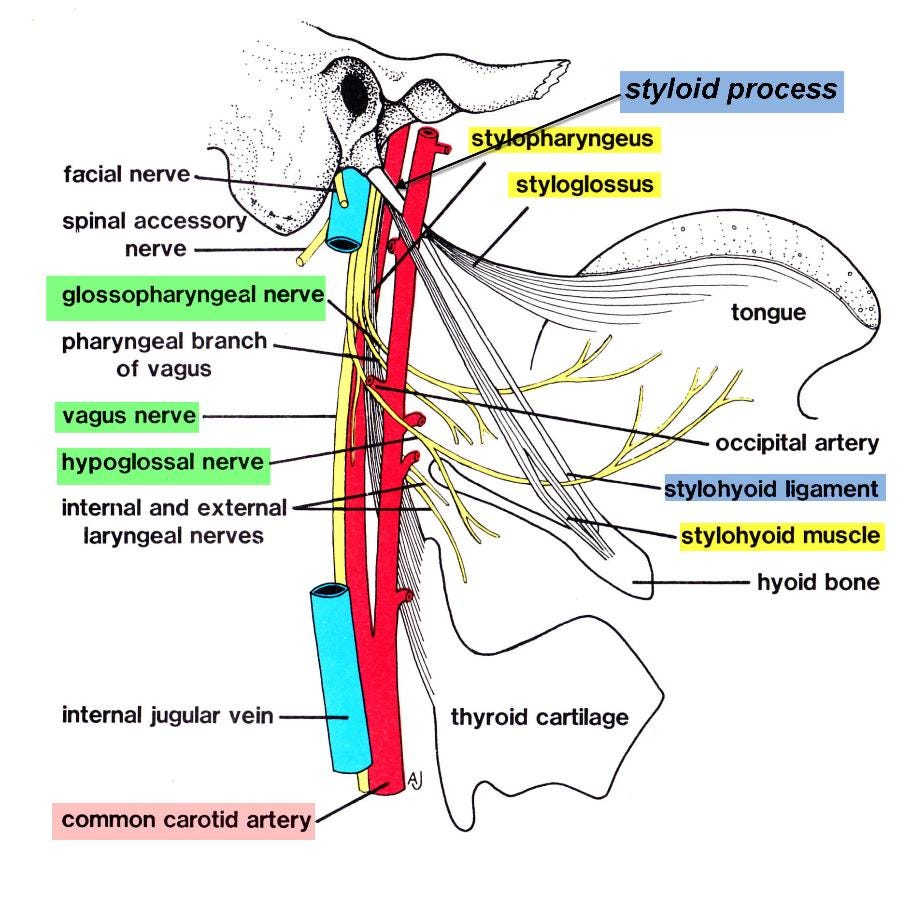
This is due to asymmetry in the vagus nerve contribution to heart function.1 Only the right actively slows heartrate. In other words, despite two nerves, the innervation of structures by the RLN is not symmetrical. In my case, this sign was dismissed as anxiety, a form of medical gaslighting.
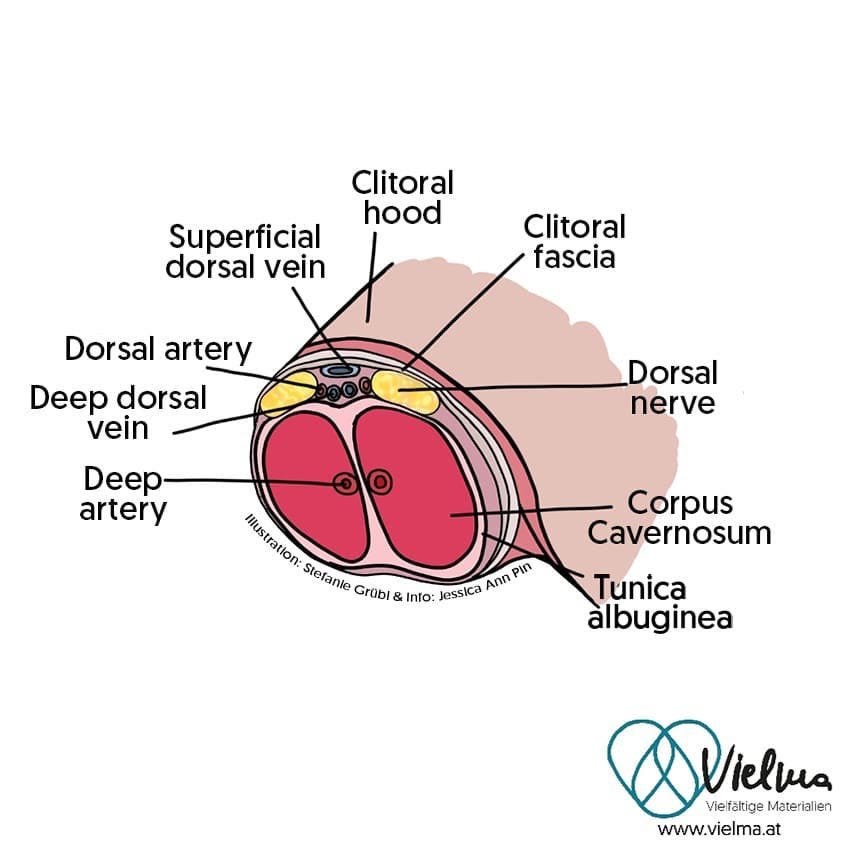
Have any of these doctors asked the question of whether one dorsal clitoral nerve is more significant to clitoral function than the other? Or are we just assuming we know everything there is to know about female anatomy and physiology, when they barely started including anatomical drawings of the relevant structures in surgical textbooks within my lifetime?
Are these girls and women too ashamed to admit how much of their anatomy they can no longer feel, how little it moves compared to before, even if they can "still climax" with a perhaps partially paralyzed, half numb clitoris? Did they ever achieve a level of sexual function and experience that would give a reasonable basis for comparison? If they were puberty suppressed, Dr Marci Bowers would be skeptical.
1https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3198976/
Anatomical drawings taken from here:
https://twitter.com/jess_ann_pin/status/1295773999083876353?t=5sqyh5S0No0y0Of_02w68A&s=19
Eagle syndrome drawing: https://images.app.goo.gl/KNGhJwvzUitR3vJc8
'Can you still orgasm after phalloplasty? Absolutely yes!'
Well he is absolutely lying.
Dr. Frankenpenis here needs to be incarcerated with the other sex abusers. And keep him in the men's prison, please. He and any Igor / nurse who assists with this nonsense please LOCK THEM UP. This, folks, is a goddamn butcher and I hope the day is soon that justice is served on his greedy perverted "practice". His snake oil is being sold to vulnerable and bewildered psych patients. Mutilation is not medicine.
The factitious disorder that is "gender dysphoria" is not appropriately treated, ever, with surgery. Ethical patient care does not include "affirming" delusions.
This is a man, flaunting how much he hurts women, taken to a whole other level.
I promised when his patients complain, he victim blames and then ghosts them.
And let us not miss the part where he mentions being able to orgasm if you could orgasm before. If.